

Here is a medical claim that would have sounded absurd a generation ago: lacking close friendships is roughly as dangerous as smoking fifteen cigarettes a day. That comparison, drawn from a meta-analysis of 3.4 million participants by Brigham Young University psychologist Julianne Holt-Lunstad, is not a metaphor or a motivational slogan. It is a statistical finding, replicated across dozens of studies and now cited by the U.S. Surgeon General as a public health emergency. Social isolation increases mortality risk by 29 percent. Loneliness increases it by 26 percent. And living alone, absent other social contact, increases it by 32 percent. These numbers are comparable to, and in some cases exceed, the mortality risks associated with obesity, physical inactivity, and air pollution.
What makes these findings so striking is not just their magnitude but their mechanism. For decades, the health benefits of social connection were attributed to behavioral explanations: friends encourage you to exercise, remind you to see a doctor, keep you from drinking alone on Tuesday nights. Those explanations are true, but they are incomplete. Research published in the last few years has revealed something more fundamental. Social connection and social isolation operate directly on the body's inflammatory and stress response systems. Loneliness doesn't just make you sad. It makes you inflamed. And that inflammation, sustained over months and years, is one of the primary biological drivers of heart disease, diabetes, cognitive decline, and early death.
Your Body on Loneliness
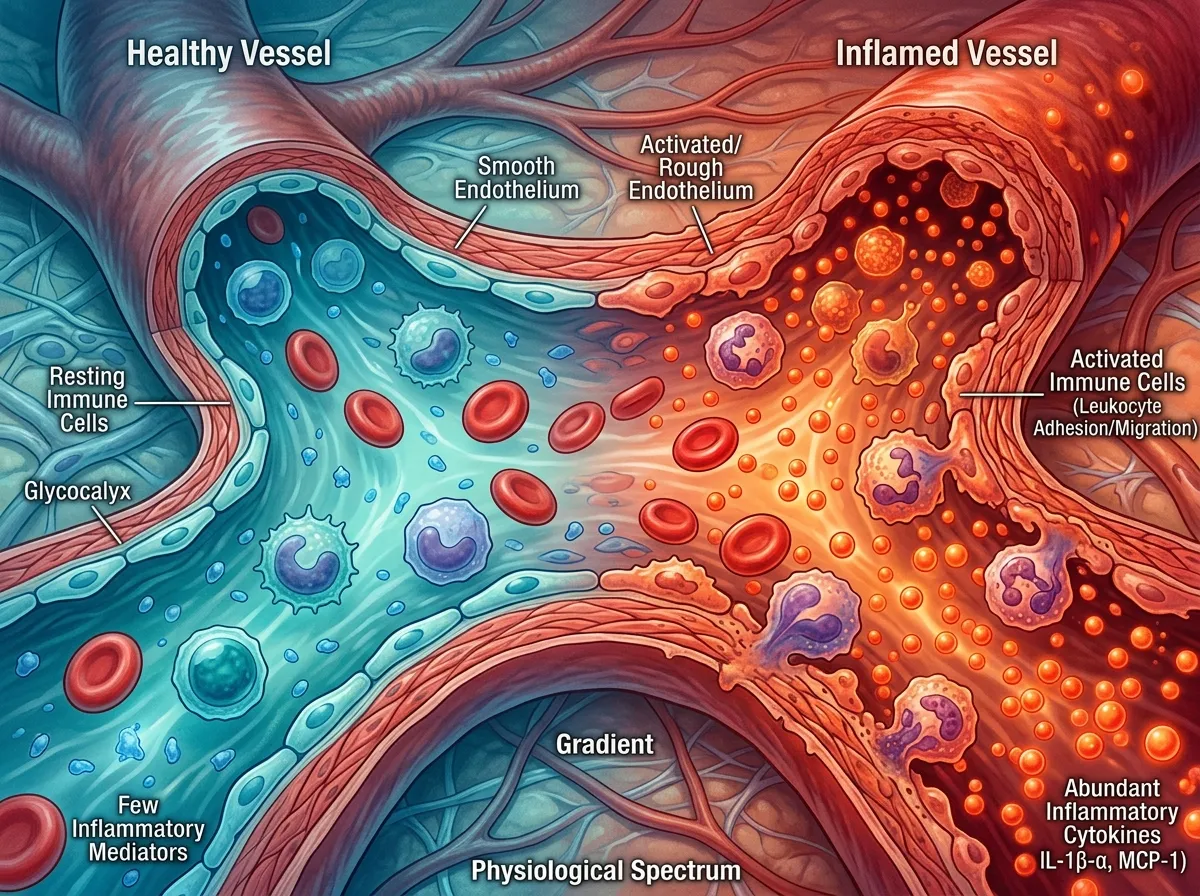
The biological story of social isolation begins with the immune system, specifically with a set of molecular signals called inflammatory biomarkers. The most commonly measured are C-reactive protein (CRP) and interleukin-6 (IL-6), both of which rise in response to infection, injury, or chronic stress. In a healthy body, inflammation is a temporary repair response. Something goes wrong, the immune system mobilizes, the problem gets fixed, and inflammation subsides. But in a lonely body, something different happens. The alarm stays on.
A landmark multi-cohort study published in Brain, Behavior, and Immunity in 2024, led by Timothy Matthews and colleagues, examined this pattern across three populations: 6,144 medical patients in Denmark, 881 adults in New Zealand, and 1,448 young adults in the United Kingdom. The results were consistent across all three groups. Socially isolated individuals showed elevated levels of inflammatory biomarkers, particularly a marker called suPAR (soluble urokinase plasminogen activator receptor), which tracks chronic systemic inflammation more reliably than the acute-phase markers CRP and IL-6. People living alone in the Danish cohort had median suPAR levels of 5.2 nanograms per milliliter, compared to 4.2 for those living with others. That difference, sustained over years, translates into meaningfully higher risk for cardiovascular disease, metabolic dysfunction, and accelerated aging.
Perhaps most unsettling was the study's longitudinal finding: social isolation measured in childhood predicted elevated inflammation in adulthood, even after controlling for lifestyle factors, depression, and medication use. The body, it appears, keeps a biological record of early social deprivation, one that continues to shape health outcomes decades later.
The Stress Architecture of Isolation
Inflammation is only one channel through which loneliness damages the body. The other is the stress response system, particularly the hypothalamic-pituitary-adrenal (HPA) axis, which regulates cortisol production. In a socially connected person, cortisol follows a predictable daily rhythm: it spikes in the morning to promote alertness and declines through the afternoon and evening. In chronically lonely individuals, this rhythm flattens. Cortisol stays elevated longer, declines less at night, and responds more dramatically to minor stressors.
The consequences ripple outward. Sustained cortisol elevation suppresses immune function (paradoxically, while also driving inflammation through separate pathways), disrupts sleep architecture, impairs memory consolidation, and promotes visceral fat storage. It is, in effect, the body running a low-grade emergency protocol at all times, diverting resources from maintenance and repair toward threat detection. The brain of a lonely person processes social information differently too, showing heightened amygdala activation in response to perceived social threats. This creates a vicious cycle: isolation makes the brain more threat-sensitive, which makes social interaction feel more risky, which deepens isolation.
This is not a matter of personality or preference. Research by John Cacioppo, the late University of Chicago neuroscientist who pioneered the study of loneliness, demonstrated that social isolation triggers evolutionary alarm systems that evolved to protect early humans from the dangers of separation from the group. For our ancestors, being alone meant vulnerability to predators, starvation, and exposure. The stress response to isolation is not a malfunction. It is a survival mechanism operating in a world that no longer matches its original context, not unlike how our brains' rapid-fire attention responses evolved for predators but now get hijacked by smartphone notifications.
What Blue Zones Actually Teach Us
If isolation is biological poison, the antidote has been hiding in plain sight for decades, embedded in the lifestyle patterns of the world's longest-lived populations. The Blue Zones, regions identified by National Geographic Fellow Dan Buettner where people routinely live past 100, include Sardinia in Italy, Okinawa in Japan, Nicoya in Costa Rica, and Ikaria in Greece. A peer-reviewed study published in The Gerontologist in December 2025, authored by Steven N. Austad, PhD, Scientific Director of the American Federation for Aging Research, and Giovanni Mario Pes, MD, confirmed the scientific validity of Blue Zones longevity data after years of skepticism from some demographers.
What these regions share is not a single dietary trick or exercise regimen. It is an architecture of daily social contact. In Okinawa, people form "moai," small social groups that meet regularly throughout life, providing emotional support, financial assistance, and accountability. In Sardinia, multigenerational households remain the norm, meaning older adults maintain daily face-to-face contact with family across age groups. In Ikaria, afternoon social gatherings over herbal tea are not optional leisure but structural features of community life.
The Blue Zones research makes a point that often gets lost in the longevity conversation: social connection is not one item on a checklist alongside diet, exercise, and sleep. It is the infrastructure that makes all the other behaviors sustainable. People in Blue Zones walk more, eat better, and sleep more consistently not because they have superior willpower but because their social environments make those behaviors the default. The science of habit formation confirms this principle: behaviors embedded in social context persist far longer than those maintained through individual discipline alone.

The 2026 Longevity Conversation
The science of social connection is intersecting with a broader cultural shift. In its annual wellness trends report, the Global Wellness Summit identified 2026 as the year wellness moves from individual optimization toward collective, human-centered experiences. The "festivalization of wellness," as the report calls it, reflects a backlash against the isolated, metrics-driven approach that dominated the previous decade: tracking sleep scores alone, optimizing macros in solitude, meditating with an app instead of a group. A parallel survey by Life Time, the fitness and wellness company, found that 82 percent of respondents plan to focus more on overall health and wellbeing in 2026, with 37.8 percent identifying longevity as the wellness trend most likely to define the year.
But the longevity conversation in 2026 has a notable gap. Much of the popular discourse centers on interventions that are individual and often expensive: GLP-1 medications, NAD+ supplements, cold plunge protocols, continuous glucose monitors. These tools have real value for specific populations, but they address longevity through a biomedical lens that largely ignores the social determinants that decades of research have shown to be equally important. One in five U.S. adults has reportedly used GLP-1 drugs, according to recent survey data. Meanwhile, roughly half of American adults report experiencing loneliness, a risk factor whose mortality impact rivals or exceeds many of the conditions those drugs are designed to treat.
This is not an argument against medical innovation. It is an observation about where attention and resources flow. The biological pathways through which social connection protects health, reduced inflammatory signaling, normalized cortisol rhythms, improved cardiovascular regulation, enhanced immune surveillance, are as well-documented as the mechanisms behind most pharmaceutical interventions. Yet there is no venture capital funding for "having dinner with friends three times a week," no wearable that tracks the quality of your conversations, no subscription service for the kind of daily, low-stakes social contact that Blue Zones populations have maintained for generations.
Building the Infrastructure of Connection
If the research is this clear, why is loneliness still worsening? Part of the answer is structural. The built environment of most American communities actively discourages casual social contact. Suburban sprawl separates homes from gathering places. Car-dependent design eliminates the walking and public transit interactions that create incidental social encounters. The decline of "third places," the cafes, barbershops, community centers, and religious institutions that sociologist Ray Oldenburg identified as essential to social life, has removed the physical infrastructure where loose social ties once formed naturally.
The response is emerging from unexpected directions. Fitness communities are evolving into what some researchers call "intentional third spaces," environments designed around physical activity that also function as social hubs. Group walks, communal cooking events, and breathwork sessions are proliferating not because walking, cooking, or breathing are new activities but because organizing them as group experiences addresses a need that individual practice cannot. The Global Wellness Summit notes that women in particular are "turning from lonely fitness to empowering sports," choosing team-based activities over solo gym sessions, a shift driven less by exercise science than by the recognition that working out alongside others feels fundamentally different from working out alone.
The neuroscience supports this intuition. Exercise performed in groups triggers greater endorphin release than the same exercise performed solo, a phenomenon sometimes called the "social endorphin hypothesis." Group physical activity also promotes synchronization of movement and breathing, which research has linked to increased feelings of trust and social bonding. The runner who joins a local running club and the CrossFit member who keeps showing up at 6 a.m. are not just building cardiovascular fitness. They are building the kind of repeated, low-barrier social contact that the loneliness research identifies as protective, the kind of contact that, over years, becomes an automatic habit woven into the structure of daily life.
From Individual Fix to Collective Design
In May 2023, U.S. Surgeon General Vivek Murthy issued a formal advisory declaring loneliness a public health epidemic, framing social disconnection not as a personal failing but as a systemic crisis requiring coordinated intervention. The advisory compared the health impact of loneliness to smoking fifteen cigarettes daily and called for a national strategy built on six pillars, including strengthening social infrastructure, reforming digital environments, and investing in research. The advisory was notable for its framing: it treated social connection not as a lifestyle preference but as a biological necessity, comparable in importance to clean water, nutritious food, and physical safety.
That framing matters because it shifts responsibility. If loneliness is a personal problem, the solution is personal: download a friendship app, join a club, try harder. If loneliness is a public health crisis shaped by structural forces, the solutions need to operate at the structural level too. Urban planning that prioritizes walkability and mixed-use development creates more opportunities for incidental social contact. Workplace policies that allow flexible scheduling create more time for community involvement. Healthcare systems that screen for social isolation alongside blood pressure and cholesterol catch a risk factor that is, by the numbers, equally dangerous.
Some of this is already happening. The 2025 validation of Blue Zones research by Austad and Pes in The Gerontologist has given public health advocates new ammunition for community-level interventions. Several U.S. cities have begun experimenting with "social prescribing," a model borrowed from the United Kingdom's National Health Service in which doctors literally prescribe social activities, group art classes, walking groups, volunteer work, as part of treatment plans for patients with chronic conditions. Early data from these programs shows measurable reductions in healthcare utilization and improvements in self-reported wellbeing.

The Bigger Picture
There is something almost embarrassingly simple at the center of this research. After decades of studying inflammation biomarkers, cortisol rhythms, proteomic signatures, and mortality statistics, the finding reduces to a truth that most people already sense intuitively: being around people who care about you is good for your health, and being chronically alone is bad for it. The contribution of the science is not the insight itself but the precision with which it quantifies what that insight means, and the urgency it creates for treating social connection as infrastructure rather than luxury.
The biology is unambiguous. Social isolation elevates inflammatory markers, dysregulates stress hormones, accelerates cellular aging, and increases mortality across every demographic studied. Social connection does the opposite: it lowers inflammation, normalizes cortisol, strengthens immune function, and adds years to life. These effects operate independently of diet, exercise, income, and access to healthcare. They are not confounds or correlations waiting to be explained away by some hidden variable. They are causal pathways, confirmed through longitudinal studies, multi-cohort analyses, and proteomic research mapping the molecular signatures of isolation across thousands of plasma proteins.
What remains is the question of whether a society organized around individual optimization can reorganize itself around collective wellbeing. The longevity industry in 2026 is projected to grow into a multi-trillion-dollar market, driven primarily by supplements, drugs, devices, and personalized protocols. None of that is wasted, but the evidence suggests that the most powerful longevity intervention available is also the oldest and the cheapest. It does not require a prescription, a subscription, or a laboratory. It requires showing up, repeatedly, in the company of people who know your name. The research on flow states and optimal experience tells us that the deepest human satisfaction comes from full engagement with meaningful activity. It turns out that the deepest human health may come from something equally straightforward: full engagement with meaningful relationships.
The Blue Zones will not last forever. Austad and Pes noted that some formerly qualifying regions have already lost their exceptional longevity status as modernization, urbanization, and the erosion of traditional social structures took hold. The lesson is not that we should romanticize pre-modern life. It is that the social architectures those communities developed over centuries, the daily rituals of shared meals, the multigenerational households, the built environments that made walking and gathering the path of least resistance, were not cultural decoration. They were, quite literally, medicine. The question for the rest of us is whether we can build that medicine back into the way we live, not as a nostalgic return to something old, but as a deliberate investment in something the science tells us we cannot afford to lose.
Sources
- Loneliness and Social Isolation as Risk Factors for Mortality: A Meta-Analytic Review - Holt-Lunstad, J., Smith, T.B., Baker, M., Harris, T., & Stephenson, D. (2015). Perspectives on Psychological Science, 10(2), 227-237.
- Social Isolation, Loneliness, and Inflammation: A Multi-Cohort Investigation - Matthews, T., Rasmussen, L.J.H., et al. (2024). Brain, Behavior, and Immunity.
- New Research Confirms the Scientific Validity of Blue Zones Longevity Data - Austad, S.N. & Pes, G.M. (2025). The Gerontologist.
- Loneliness and Social Isolation as Risk Factors: The Power of Social Connection in Prevention - Holt-Lunstad, J. (2021). American Journal of Lifestyle Medicine.
- Global Wellness Summit Releases 10 Wellness Trends for 2026 - Global Wellness Institute (2025).